Dr Smallman discusses the anatomy of the anterior compartment of the knee with a view to relating it to the symptoms of anterior knee pain.
 First published 2018, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
First published 2018, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
An alternative viewpoint on anterior knee pain - course
- CLINICAL CASES - Case 4
- CLINICAL CASES - Case 5
- BACKGROUND ANATOMY - Anterior compartment of the knee
- BACKGROUND ANATOMY - The Fat Pad
- BACKGROUND ANATOMY - The Infrapatellar Plica
- BACKGROUND ANATOMY - how the fat pad and infrapatellar plica form
- BACKGROUND PHYSIOLOGY - Kinematics of the knee
- BACKGROUND PHYSIOLOGY - Knee pain in general
- TAKEHOME MESSAGE - The surgical technique of Untethering the Fat Pad
The anterior compartment is a geometric space containing linked structures that together function first to simply fill the space, and then to act as a hydraulic shock absorber.
The structures are the fat pad and infrapatellar plica (IPP) - which we call the 'IPP-fat pad complex' - and they together fill the space, whose borders change as the knee moves, requiring that the fat pad be semi-liquid and completely deformable, and it is...
The geometry of the Anterior Compartment and the link to AKP
The global message of this course is to try to correlate structure and function to the clinical problem of Anterior Knee Pain so that it all makes sense.
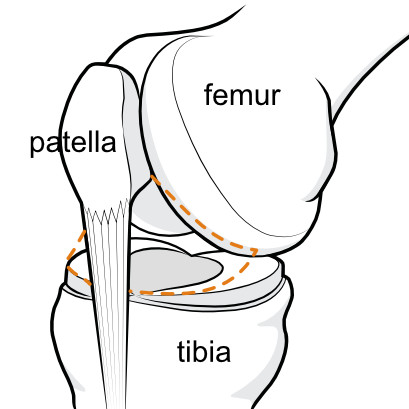 Figure 1A. Illustration outlining the geometric boundaries of the anterior compartment, more or less in line with Figure 1B but in 1B the patella has been turned down out of view. Figure 1A. Illustration outlining the geometric boundaries of the anterior compartment, more or less in line with Figure 1B but in 1B the patella has been turned down out of view. |
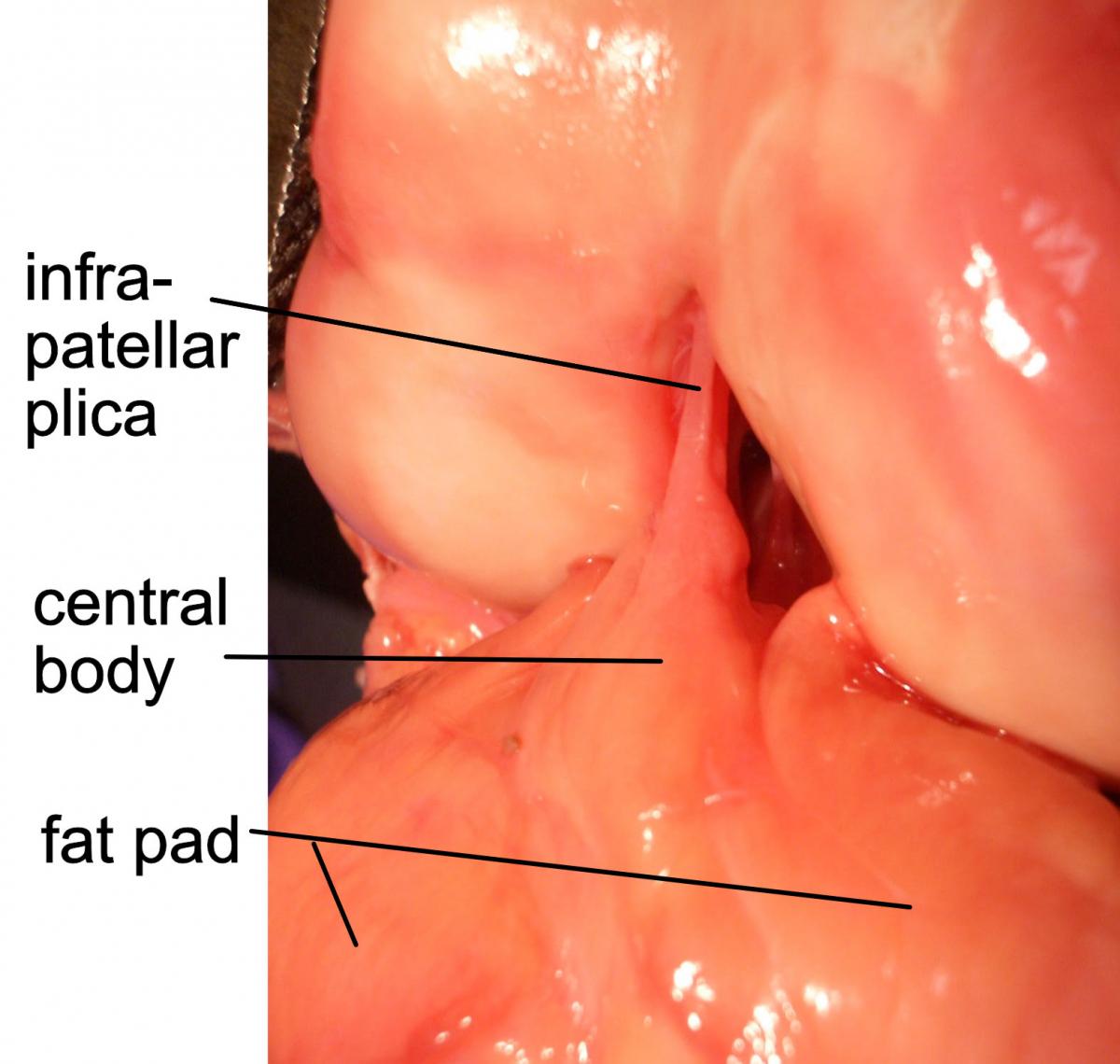 Figure 1B. A great shot from an anatomic dissection that opens up the anterior compartment showing the unit that is the fat pad and infrapatellar plica. Figure 1B. A great shot from an anatomic dissection that opens up the anterior compartment showing the unit that is the fat pad and infrapatellar plica. |
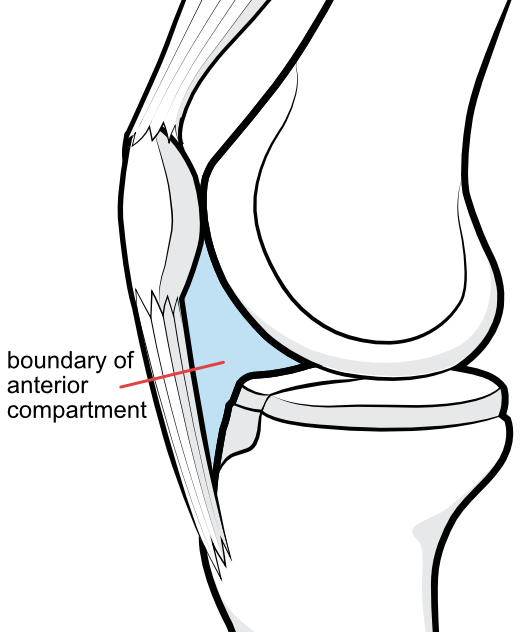 |
Figure 1C. The boundaries of the space are soft tissue in front, and in a small area in the middle of the otherwise bony back wall. Rigid bone makes up the rest of the margin: the knee-cap or patella in front, the femur above and behind, and the tibia below. These bones have complex geometry. The semi-liquid fat pad deforms to fill this space as the knee moves |
Palpating the Anterior Compartment
The soft tissue front boundary of the anterior compartment is dense, firm fibrous tissue that wraps, like a hood, around the front of the knee below the patella. This sheet of fibrous tissue is thicker in the middle where it is named the patellar tendon, which attaches to the bony prominence of the tibia below. On either side, the capsule is simply a firm sheet of dense connective tissue which projects as a prominence on either side as the knee extends fully. Firmly attached to the inner surface of the patellar tendon and the capsule on either side is the fat pad. The prominence and firm, rubbery feel reflect the nature of the underlying fat pad.
When the knee flexes to 90 degrees, the fat pad retracts somewhat and the prominence becomes a recess that you can feel on either side of the mid-line prominence of the patellar tendon. The capsule of any movable, or synovial joint is a closed sack of fibrous tissue, completely enclosing the joint, consisting of an outer fibrous protective layer, and an inner synovial layer, which produces the viscous synovial fluid liquid, the lubricant for friction-free motion and nourishment of the shock absorbing cartilage that cloaks the joint surfaces of the bones.
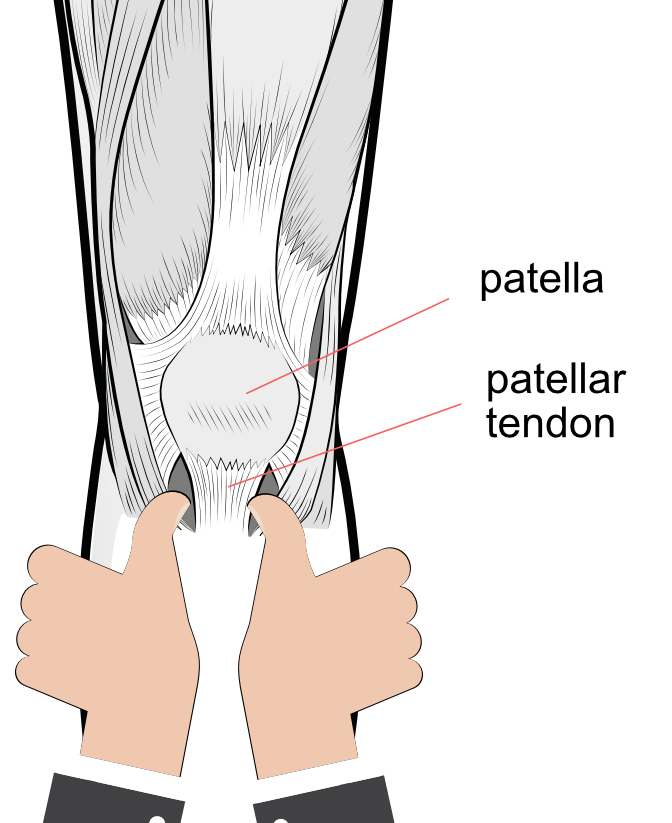 |
Figure 1D. The physician supports the patient's leg between the upper arm and chest wall, leaving both hands to hold the flexed knee in mid flexion ( ~ 45 degrees). The thumbs are positioned as shown in the diagram, applying gentle pressure on the recesses below the patella on either side of the patellar tendon, as the knee is moved to full extension. A positive test is the presence of pain, felt under the thumbs suggesting that the noxious nerves in the fat pad have been activated. With pressure on the thumbs as shown, pain on either side or both, occurring as the knee is passively knee extended, is a positive Hoffa's Sign. |
PREVIOUS PART: CLINICAL CASES - Case 5
NEXT PART: BACKGROUND ANATOMY - The Fat Pad
Dr Thomas Smallman

Dr Smallman is a board-certified orthopaedic surgeon with special expertise in the diagnosis and treatment of ...read more