The ligamentum mucosum or infrapatellar plica seems to play a role in anterior knee pain.
 First published 2018, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
First published 2018, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
An alternative viewpoint on anterior knee pain - course
- CLINICAL CASES - Case 4
- CLINICAL CASES - Case 5
- BACKGROUND ANATOMY - Anterior compartment of the knee
- BACKGROUND ANATOMY - The Fat Pad
- BACKGROUND ANATOMY - The Infrapatellar Plica
- BACKGROUND ANATOMY - how the fat pad and infrapatellar plica form
- BACKGROUND PHYSIOLOGY - Kinematics of the knee
- BACKGROUND PHYSIOLOGY - Knee pain in general
- TAKEHOME MESSAGE - The surgical technique of Untethering the Fat Pad
The infrapatellar plica (IPP) is structure that connects the fat pad to the femur bone.
It is a floppy, distensible band of soft tissue - part of the IPP-fat pad complex - tethering the fat pad to bone and anchoring the complex to the apex of the notch as the knee moves. It contains dense connective tissue (including collagen which defines it as a ligament and elastin, allowing it to stretch easily), loose connective tissue, fat (allowing compressible shock absorption), and supporting vessels and nerves. It sits in front of and parallels the anterior cruciate ligament (ACL). Although it is classifiable as a ligament it is unusual in being non-isometric, which means that its dimensions change as the knee moves.
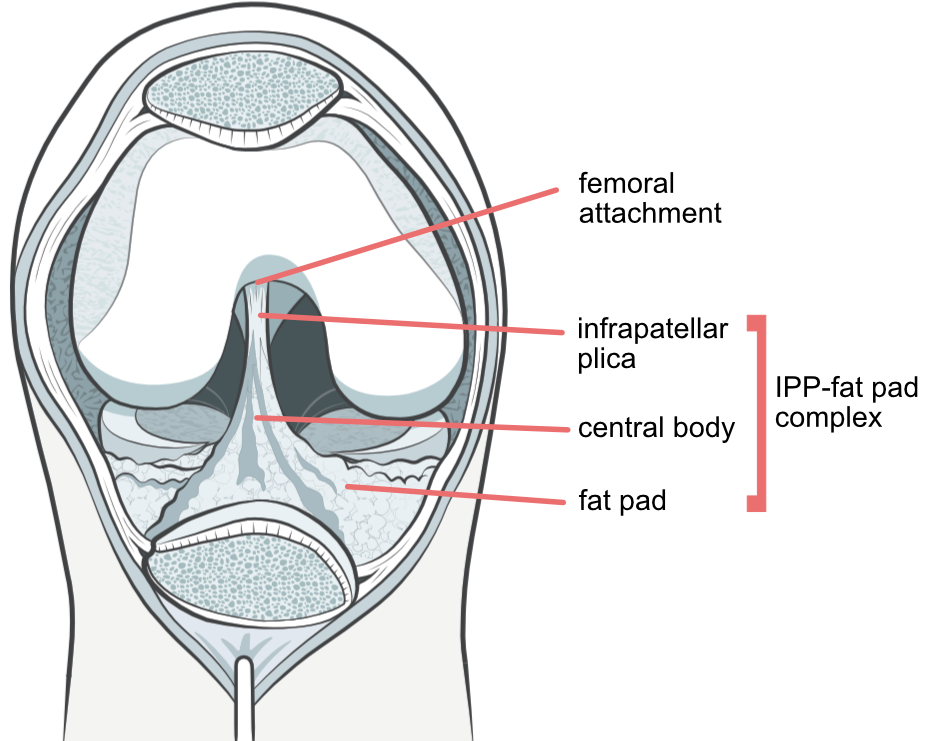
Figure 5.
In this illustration - a bit different from the dissection photographs of the previous section - the patella has been cut in half and the bottom half bent down. You should now be able to identify the fat pad, infrapatellar plica, central body and the femoral attachment of the infrapatellar plica. The central body is part of the fat pad that attaches it to the infrapatellar plica and functionally attenuates the forces between these two structures - it is considered to be a transition zone. When present, the IPP partially obscures the cruciate ligaments, and its anatomy is not easily appreciated during normal arthroscopic surgery.
Mechanical behaviour of the IPP during knee motion
This arthroscopic video is associated with Case 3. Viewing from the anterolateral portal one sees the contents of the anterior compartment in this adolescent with chronic AKP who developed the problem abruptly, without trauma or overuse, 3 years before, early in his growth spurt. He was profoundly disabled, affected in both knees by pain that had taken over his life. Both knees underwent arthroscopy and untethering of the fat pad 3 months apart. His pain was abolished thereafter and his knees were pain free at follow-up 84 months post op.
The screenshots and legends below explain the subtle changes in appearance of the IPP that suggested that the IPP is a structure that has a mechanical function, and led to the body of research that is being demonstrated to you in this course.
 |
 |
|
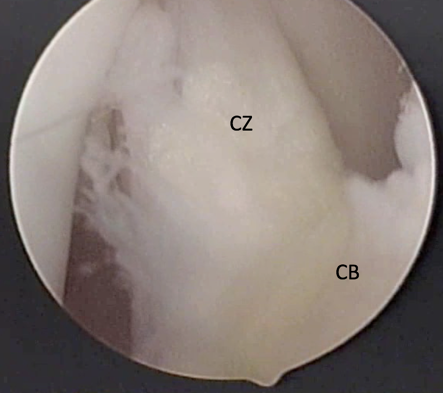
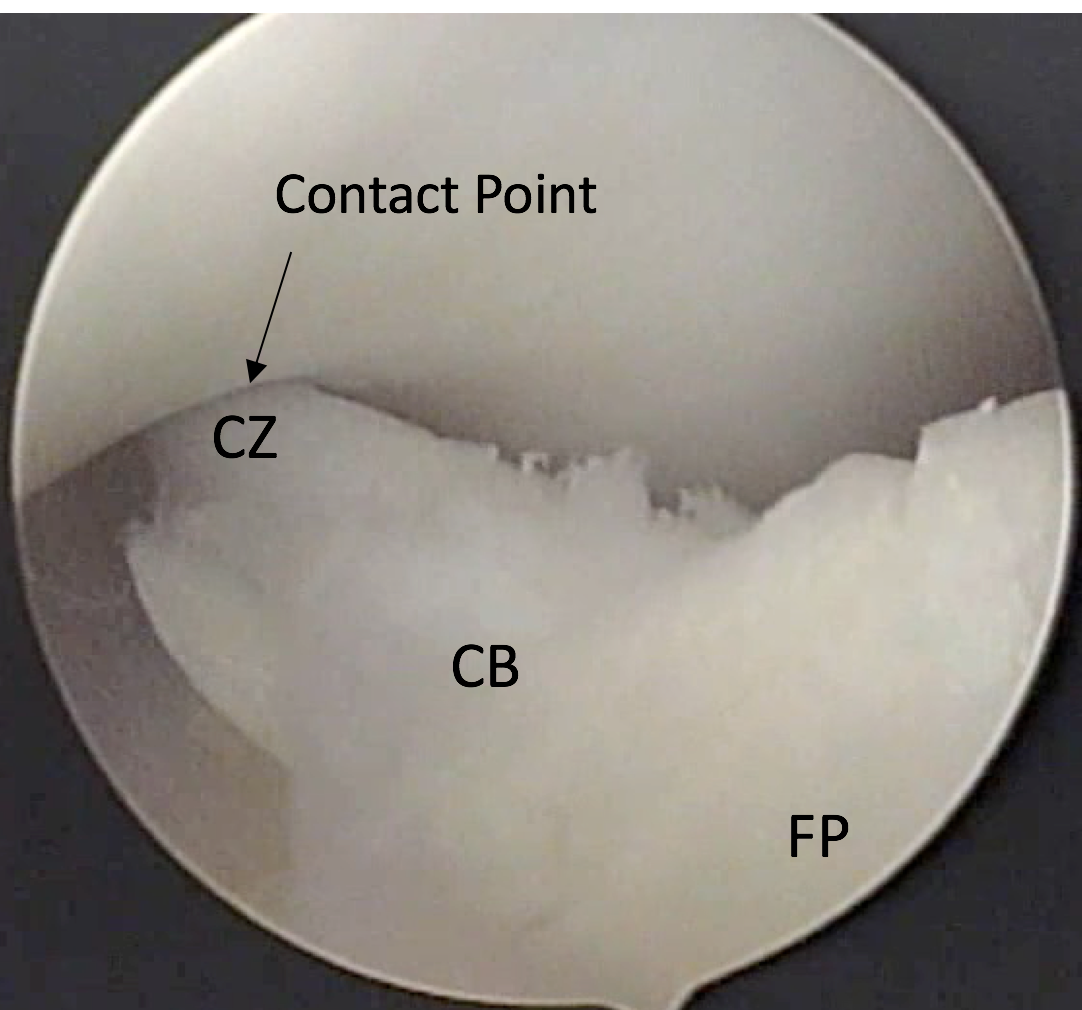
Figure 6A. Knee at 90° flexion, showing the IPP, central body, and portions of the fat pad. The IPP (CZ) is vertical, appears separate and has a leading edge that is straight, suggesting that it is under tension. |
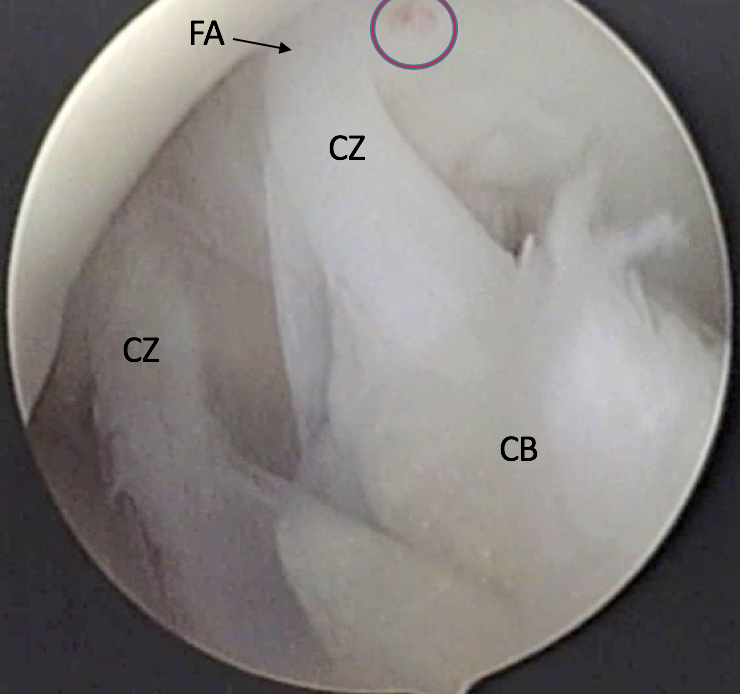
Figure 6B. Knee at 45° flexion. The IPP (CZ) is split in 2 bands, is attached to the apex of the femoral notch (FA) above, and spans the gap to the central body (CB) attachment to the fat pad. There is a zone of inflammation (circle) adjacent to FA. The central zone (CZ) is the ligament itself, the leading edge curved slightly suggesting laxity. |
 |
 |
|
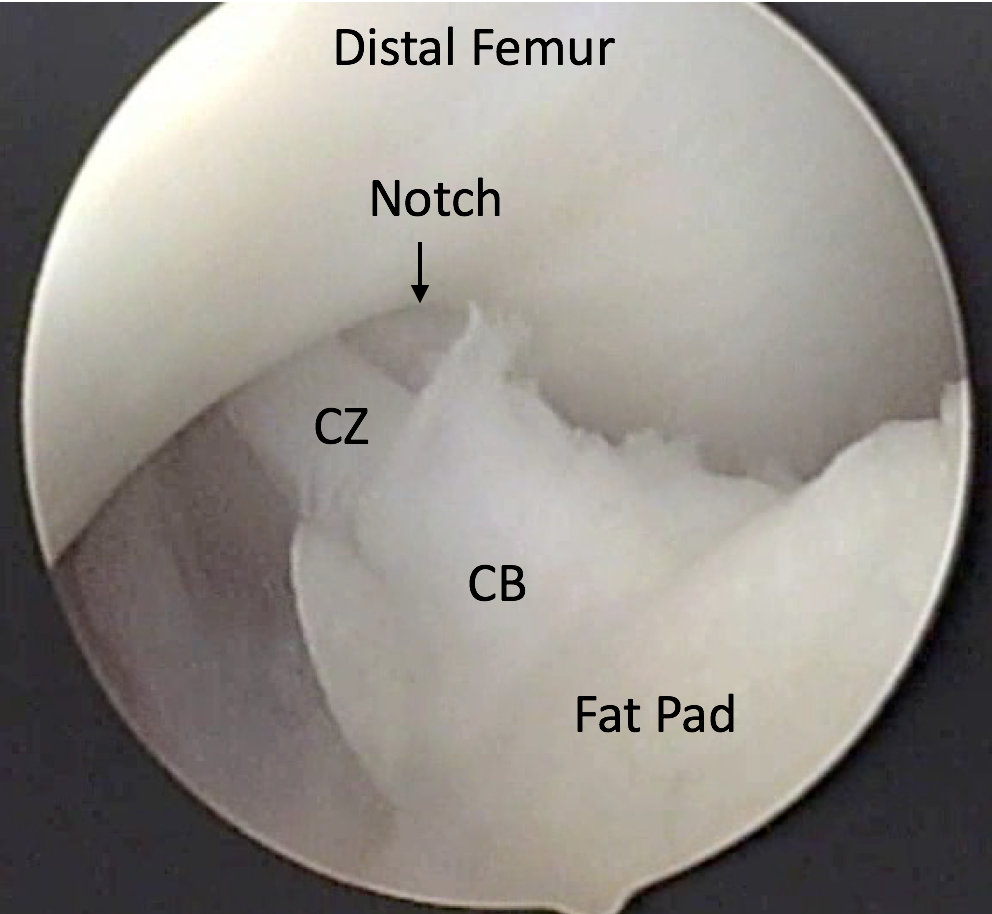
Figure 6C. Knee at ~20° flexion (approaching straight). IPP (CZ) approaches contact to the margin of the articular cartilage at the apex of the femoral notch, leading edge is straight, suggesting tension. |
Figure 6D. Knee at ~15° flexion (approaching straight). IPP (CZ) contacts notch. At this point, under the influence of the screw-home mechanism of the knee, the femur moves relatively posterior, and the tibia rotates externally and moves relatively anterior to the end of extension. This creates increasing stretch of the IPP, additive to the stretch associated with non-isometricity (this can only be seen in the kinematic videos that follow). The apex of the notch becomes a pulley at this point changing the direction and point of application of the force of the extensor apparatus. Now during further extension, the superior surfaces of the IPP, central body (B) and fat pad (FP) are subject to compression and shear forces as they are dragged around this “pulley”. This is the likely cause of “isolated” trochlear osteoarthritis. |
 |
 |
|
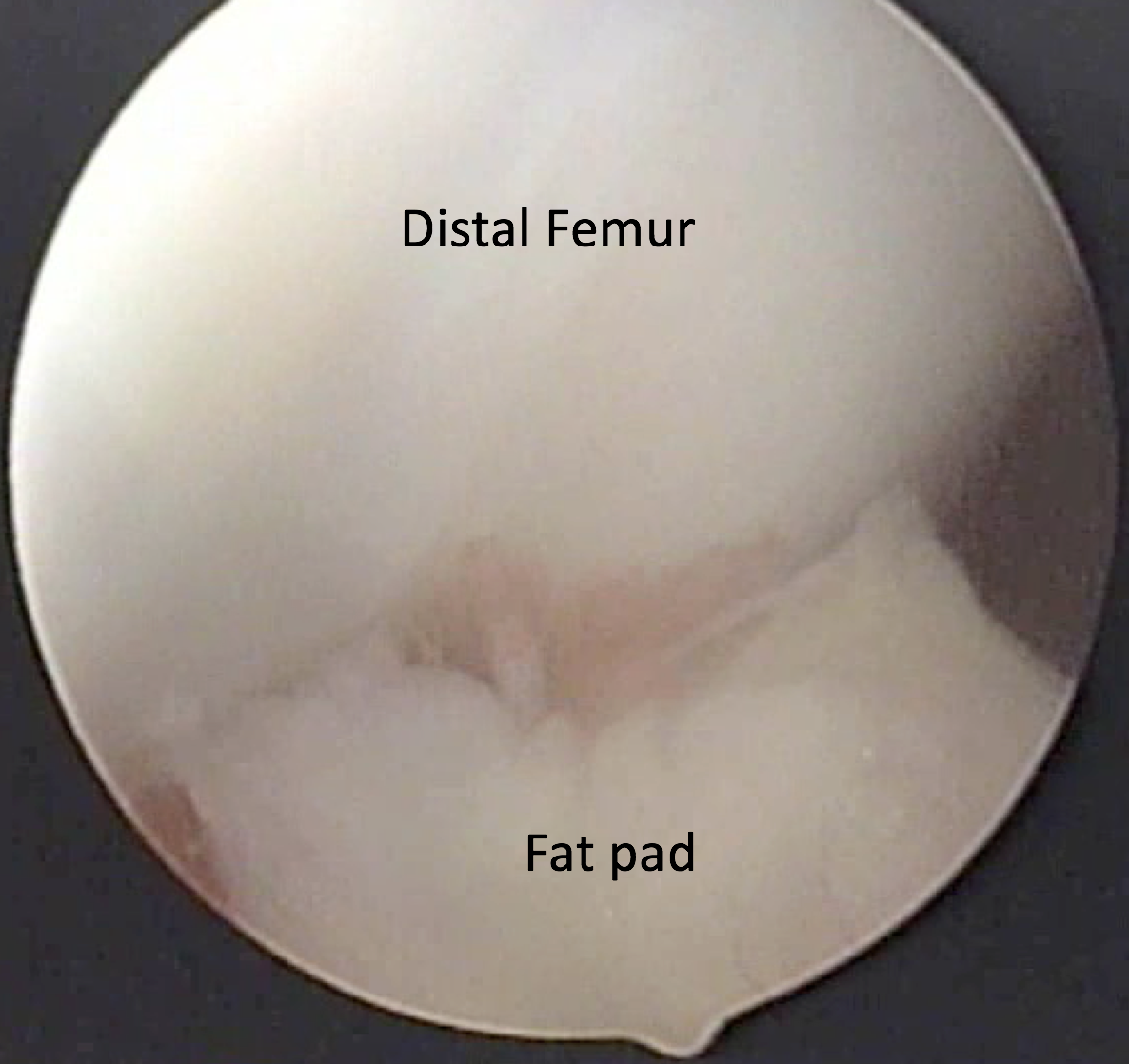
Figure 6E. Knee at ~ full extension. The view is from above. The IPP and central body have rotated out of view. The fat pad contacts the trochlea. |
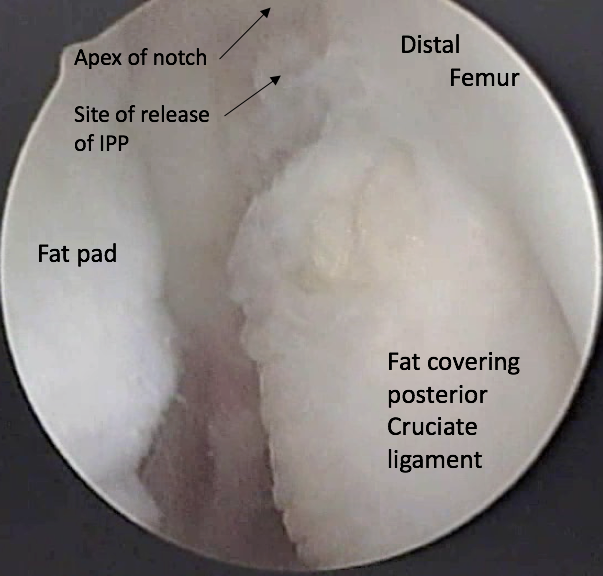
Figure 6F. Knee at ~ 90° flexion. View from the anteromedial portal. The fat pad has been released; there is no attachment between it and the distal femur. The fat pad now is unconstrained; the operation untethers the fat pad (see kinematic discussion). The patient awakens with pain from the portals and the surgery but the AKP is abolished in most, and rarely recurs. |
References
1. Kim S.J., Kim J.Y., Lee J.W. Pathologic infrapatellar plica. Arthroscopy. 2002;18:E25. [PubMed]
2. Kim S.J., Choe W.S. Pathological infrapatellar plica: A report of two cases and literature review. Arthroscopy. 1996;12:236–239. [PubMed]
3. Kim S.J., Min B.H., Kim H.K. Arthroscopic anatomy of the infrapatellar plica. Arthroscopy. 1996;12:561–564. [PubMed]
PREVIOUS PART: BACKGROUND ANATOMY - The Fat Pad
NEXT PART: BACKGROUND ANATOMY - how the fat pad and infrapatellar plica form
Dr Thomas Smallman

Dr Smallman is a board-certified orthopaedic surgeon with special expertise in the diagnosis and treatment of ...read more