Restoring stability is an important part of biological knee replacement.
 First published 2010 by Dr Kevin R Stone, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
First published 2010 by Dr Kevin R Stone, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
Biologic knee replacement - course
- Introduction to the concept of biologic knee replacement
- Articular cartilage repair or regrowth
- Partial meniscectomy, meniscal repair, reconstruction or replacement
- Options for damaged knee ligaments in biologic knee replacement
- Osteotomy as an adjunct procedure to biologic knee replacement
- Video - The paste graft technique
- Video - Meniscus cartilage replacement for arthritis
- Video - Lateral meniscus allograft transplantation
- Videos - Knee Dislocation: ACL Reconstruction - PCL Reconstruction / Reconstruction of posterolateral corner
- Treatment of failed Osteochondritis Dissecans repair by Articular Cartilage Paste Grafting
- Combined Meniscus Allograft Transplantation and Articular Cartilage Paste Grafting
- Collagen Meniscus Implant
For the unstable knee where there has been ligament damage such as an ACL tear, a PCL tear, a posterolateral corner tear or a medial collateral ligament (MCL) tear – which are the most common injuries that we see – we want to stabilise that joint as part of any biologic knee reconstruction.
We approach that in the following way –
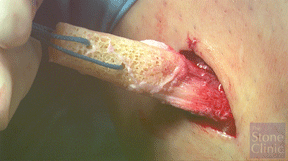
We have posted a video called ‘Knee dislocation, reconstruction of the ACL, PCL and posterolateral corner' on our website for people to see, but in general we will use a sterilised bone patellar-tendon bone allograft (photo on right) for the ACL and for the PCL, and for the posterolateral corner we will use a sterilised anterior tibialis tendon which we pass through the fibular head, underneath the skin and underneath the iliotibial band and up to a small incision through the iliotibial band to the anatomic insertion site.
For reconstruction of ruptured ligaments in the knee when we are doing a biological joint reconstruction, we don’t want to sacrifice any of the patient’s own tissue if it is not necessary. Up until about 5 years ago we felt as though allograft tissues were not as reliable as autograft tissues.
Once we were able to obtain sterilised allograft tissues whose biomechanical properties had not been damaged by the sterilisation process then we felt comfortable moving forward to use those tissues in replacement of autogenous tissues. We did not want to ‘rob Peter to pay Paul’, that is we did not want to damage one part of the knee in order to rebuild another part of the knee. Over the last 5 years our results of allograft tissue have matched our autograft tissue except that the patients have much less pain and a much faster rehabilitation.
PREVIOUS PART: Partial meniscectomy, meniscal repair, reconstruction or replacement
NEXT PART: Osteotomy as an adjunct procedure to biologic knee replacement
Dr Kevin Robert Stone

Kevin Robert Stone, M.D. is an orthopedic surgeon, who specializes in sports medicine and injuries of the knee, shoulder, and ankle joints. He has lectured and is recognized internationally as an authority on cartilage and meniscal growth, replacement, and repair. Stone is known for his development of the paste grafting...read more