Collateral ligament injuries of the knee are common, either in isolation or in combination with damage to the meniscus or cruciate ligament or capsule.
 Page updated March 2024 by Dr Sheila Strover (Clinical Editor)
Page updated March 2024 by Dr Sheila Strover (Clinical Editor)
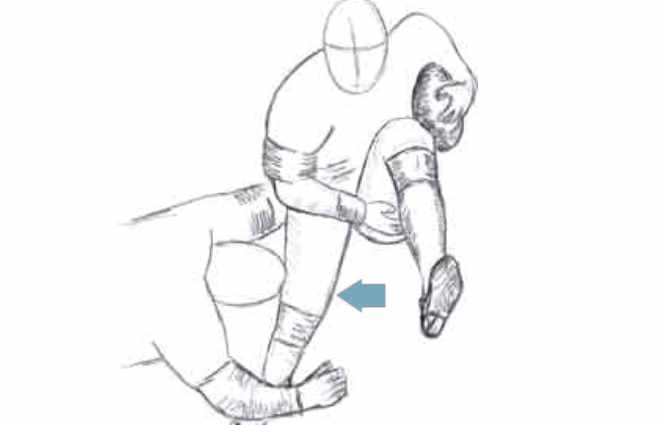
The illustration shows a sudden valgus force (knee angled inwards), and it is the medial collateral ligament (on the inner aspect of the knee) which will be damaged.

The ligament on the inner aspect is the 'medial collateral ligament' and the one on the outer aspect is the 'lateral collateral ligament'.
Mechanisms of collateral ligament injury
The mechanisms of injury include:
- a direct contact blow on the side of the knee while the foot is 'planted' (on the ground). This forces the joint to bend sideways ('varus' or 'valgus' force) and tears the ligament on the opposite side.
- landing badly from a jump so that the knee is forced sideways by the weight of the body.
How the surgeon assesses the collateral ligaments
Diagnosis of collateral ligament injury is made after the clinician takes the history of the injury and examines the knee.
Imaging methods may be used to confirm the diagnosis.
The 'history' may be one of contact or non-contact injury, but in either there is usually a sudden excessive varus or valgus force (forcing the knee into a sideways bend).
If the collateral is torn, rather than just sprained, an audible 'pop' may be heard. Pain is immediate, and experienced over the site of the ligament, but the patient may be able to continue to bear weight on that leg, albeit with bent knee, with the pain tending to increase with time.
The examination findings will differ depending on the nature and extent of the injury. With a sprain, there is tenderness over the ligament, but the joint line does not open up when the surgeon applies stress to try and bend it sideways (varus or valgus stress). In a partial tear the joint opens slightly, but in a complete tear there may be more than 10mm of opening when the varus or valgus stress is applied.
Quite often there is bruising over the ligament. In contact injury, the force may actually have been applied at the opposite side of the knee to the area of pain and bruising. Local swelling is common.
If the whole joint has swollen up, it is likely that the anterior cruciate has gone, too, and that there is blood in the joint. A knee surgeon's advice should be sought, and the postero-lateral corner carefully evaluated - as other important structures at the back of the knee may have been damaged.
Grading of collateral ligament injuries
Grade I collateral ligament tear
There is tenderness at site of injury but no opening up when stress is applied
Grade II collateral ligament tear
There may be severe discomfort and up to 5mm opening up when stress is applied
Grade III collateral ligament tear
There may be marked pain, instability and swelling, with joint opening up to 10mm when stressed
Complex injury involving the collateral ligaments
When several structures are damaged, decisions about the collateral ligament become more important. A collateral ligament may be injured together with other structures such as the cruciate ligament or the meniscus. In fact collateral ligament tears are rarely found in isolation.
A high proportion of medial collateral tears are associated with anterior cruciate ligament tears. A MCL tear in conjuction with an ACL tear and a medial meniscus tear is called the 'unhappy triad of O'Donoghue'.
Lateral collateral ligaments may be part of 'postero-lateral' corner insufficiency - which usually involves any or all of the capsule in this region, the popliteus tendon, the arcuate ligament and the cruciates.
Management of collateral ligament damage
Most collateral ligament injuries will heal themselves with rest and bracing.
Like all soft tissue injuries of the knee, the first line of management immediately after the injury is the 'PRICE' regime:
- P = protect
- R = rest
- I = ice
- C = compression
- E = elevation
Surgery, if indicated, is usually uncomplicated (stitches or staples), unless other important ligaments (like the cruciates) are damaged at the same time.